Assessing the rupture risk of abdominal aortic aneurysm based on multi-modal clinical imaging
Researchers: John Aston, Yuan Huang, Rachel Forsythe (University of Edinburgh), David Newby (University of Edinburgh), James Rudd
Abdominal aortic aneurysm (AAA) is a localized enlargement of the aorta, conventionally diagnosed when the maximum anteroposterior vessel diameter exceeds 3.0cm. AAAs are most prevalent in elderly men and are frequently asymptomatic until point of rupture, which is the catastrophic failure of the aneurysmal wall associated with an overall mortality rate between 65% and 85%. Current management is largely based on serial imaging to determine the maximum baseline diameter and rate of growth, with open or endovascular repair typically recommended for AAA measuring 5.5 cm or greater. However, clinical trials and autopsy studies suggest that some small- and medium-sized AAAs will also rupture, whereas some large aneurysms can remain static for many years. Thus, aneurysm diameter alone cannot reliably identify high-risk AAAs, highlighting the need of better risk stratification.
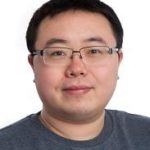
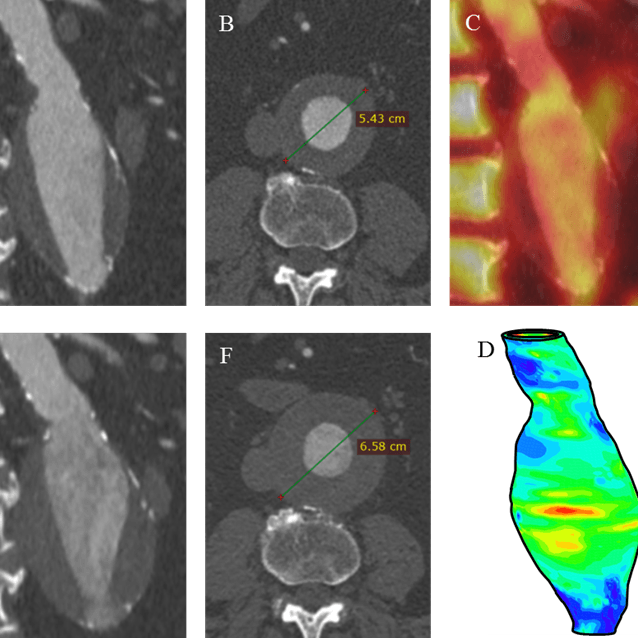
In this project, we hypothesised that, in addition to size, tissue composition and structural stress would be important predictors of growth. Thus, integrating additional variables, such as 18F-FDG PET to measure inflammation and deriving stress maps to quantify the biomechanical environment 2,3, could potentially lead to better stratification and patient management. This project is conducted as two serial studies:
- To study the association between 18F-FDG PET depicted baseline inflammation and other parameters such as patient demographics, AAA morphology/composition, and biomechanical stress derived from contrast-enhanced CT.. A key finding of this study is the statistical interaction between intraluminal thrombus (ILT) ratio and stress; inflammatory response is more likely to be observed in regions where both terms are high. This study has been completed and published.
- To identify the key predictors of AAA growth rate, calculated by comparing the infrarenal volume in the baseline and 2-year follow-up CT scans. Predictors include baseline demographics, AAA morphology/composition, biomechanical stress and 18F-FDG PET depicted inflammation. This study is ongoing.